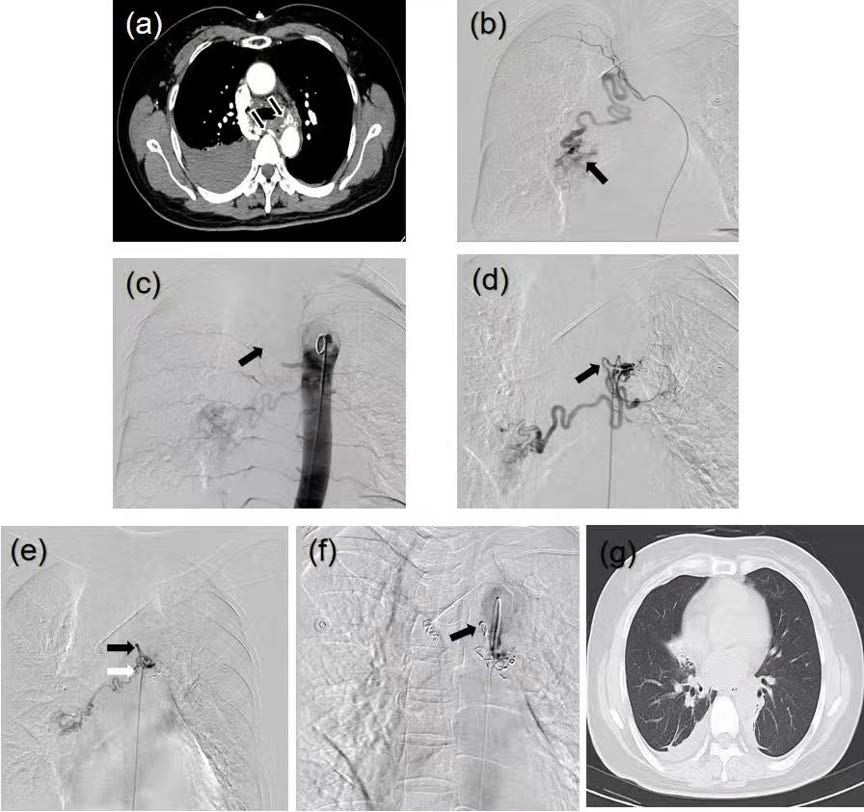
Bronchial Artery Embolization for Hemoptysis: Two Cases of Primary Bronchial Artery Racemose Hemangioma
DOI:
https://doi.org/10.3941/jrcr.6147Abstract
We report two cases of primary bronchial artery racemose hemangioma (RHBA) in female patients presenting with hemoptysis as the dominant manifestation complicated by hemodynamic instability. Following a multidisciplinary team (MDT) consensus, bronchial artery embolization (BAE) was implemented as the primary intervention. Procedural success was achieved in both cases, resulting in the complete resolution of hemoptysis and hemodynamic stabilization. Postprocedural surveillance demonstrated sustained efficacy without recurrence during the follow-up period. This study validated BAE as an effective and safe first-line therapeutic approach for RHBA while further investigating the correlation between the embolization strategy and long-term clinical outcomes.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Journal of Radiology Case Reports

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
The publisher holds the copyright to the published articles and contents. However, the articles in this journal are open-access articles distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 License, which permits reproduction and distribution, provided the original work is properly cited. The publisher and author have the right to use the text, images and other multimedia contents from the submitted work for further usage in affiliated programs. Commercial use and derivative works are not permitted, unless explicitly allowed by the publisher.