Successful Treatment of Varicose Great Saphenous Vein Complicated with Acute Thrombosis by Balloon-Assisted Thrombectomy Combined with Radiofrequency Ablation: A Case Report
DOI:
https://doi.org/10.3941/jrcr.6063Abstract
Introduction:Great Saphenous Vein (GSV) varicosity is a common clinical vascular disease, frequently complicated by Superficial Venous Thrombosis (SVT). SVT may extend to the deep venous system, causing severe Venous Thromboembolism (VTE). The standard treatment for GSV varicosity with acute SVT—especially involving the Saphenofemoral Junction (SFJ)—remains controversial. Anticoagulation is the mainstream to reduce thromboembolic risk, while surgical treatment has drawbacks like significant trauma and excessive bleeding, failing to lower long-term thromboembolic incidence. This leaves gaps in optimal timing and combined regimens, with scarce evidence for alternative therapies without standard equipment. This case report describes a successful combined interventional therapy for a patient with 30-year untreated GSV varicosity and SVT, providing practical evidence.
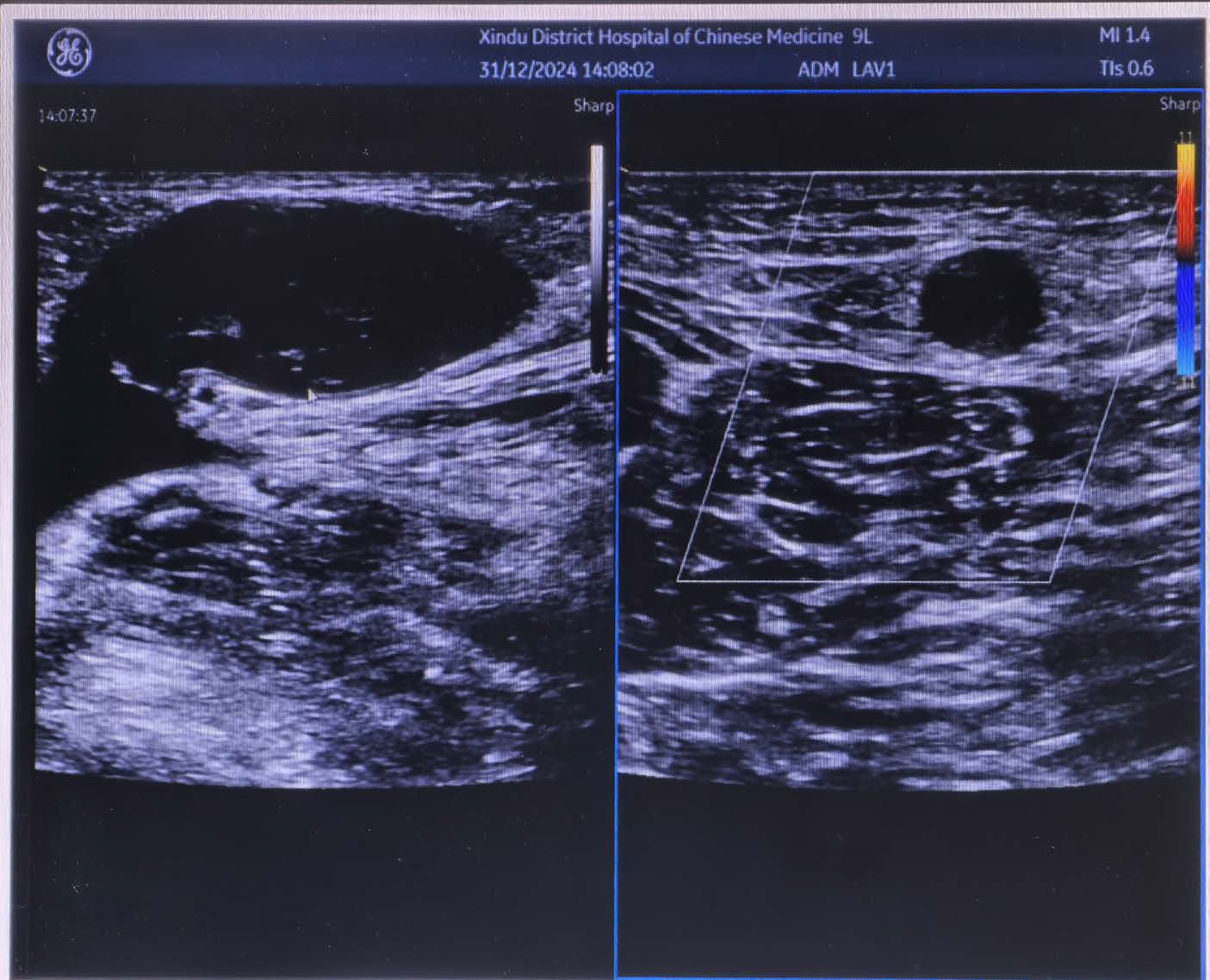
Case Study:A 74-year-old male presented with right lower limb swelling and pain for 10 days, along with 30-year untreated varicosity. Physical examination showed tortuous and dilated GSV (earthworm-like protrusions), hard nodules, erythema, edema, and ankle pigmentation (CEAP class 4; Venous Clinical Severity Score [VCSS] = 12; Aberdeen Varicose Vein Questionnaire [AVVQ] = 22). Color Doppler ultrasound confirmed extensive GSV thrombosis (extending to SFJ) without deep venous thrombosis. After full risk disclosure of VTE, the patient opted for surgery (declined vena cava filter placement). Lacking a Fogarty catheter, the operator used a deep venous balloon catheter to occlude the SFJ, performed above-knee GSV thrombectomy with a superficial venous balloon, followed by endovenous radiofrequency ablation. Below-knee tributaries were treated with ultrasound-guided foam sclerotherapy combined with minimally invasive phlebectomy. Postoperative anticoagulation relieved symptoms; 10-month follow-up showed no thrombosis recurrence, vessel recanalization, or adverse events.
Conclusion:This case demonstrates the efficacy of combined therapy (deep venous balloon occlusion, alternative catheter-based thrombectomy, radiofrequency ablation, foam sclerotherapy/minimally invasive phlebectomy) for long-standing GSV varicosity with SVT. It confirms that deep venous balloon catheters can replace Fogarty catheters in resource-limited settings. The 10-month follow-up verifies long-term safety, offering a practical treatment paradigm for similar high-risk cases and supplementing evidence for individualized GSV varicosity therapy.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Journal of Radiology Case Reports

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
The publisher holds the copyright to the published articles and contents. However, the articles in this journal are open-access articles distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 License, which permits reproduction and distribution, provided the original work is properly cited. The publisher and author have the right to use the text, images and other multimedia contents from the submitted work for further usage in affiliated programs. Commercial use and derivative works are not permitted, unless explicitly allowed by the publisher.